Qualytics ensures data quality for healthcare payers across provider files, member records, claims, and more, protecting compliance and AI.
Jun 18, 2026
8
min read
Table of Contents

In healthcare, the same data flows everywhere. Provider records, member files, claims, EDI feeds, FHIR resources, and third-party inputs move through network management, care coordination, claims adjudication, quality measurement, compliance reporting, and increasingly, AI-driven decisioning. A single record can pass through multiple handoffs and format changes before it reaches a downstream system, and at any of those transitions, an error can propagate forward without detection. When that data is incomplete, fragmented, or stale, the impact shows up as network adequacy failures, denied claims, HEDIS measure gaps, regulatory findings, and AI systems that act on the wrong information.
Most organizations still catch these problems after the fact. Traditional approaches to data quality focus on downstream detection, surfacing issues in dashboards, reconciliations, or compliance reviews after automated processes and AI systems have already acted on bad data. As automation and AI increase the speed and reach of data consumption, that risk compounds quickly.
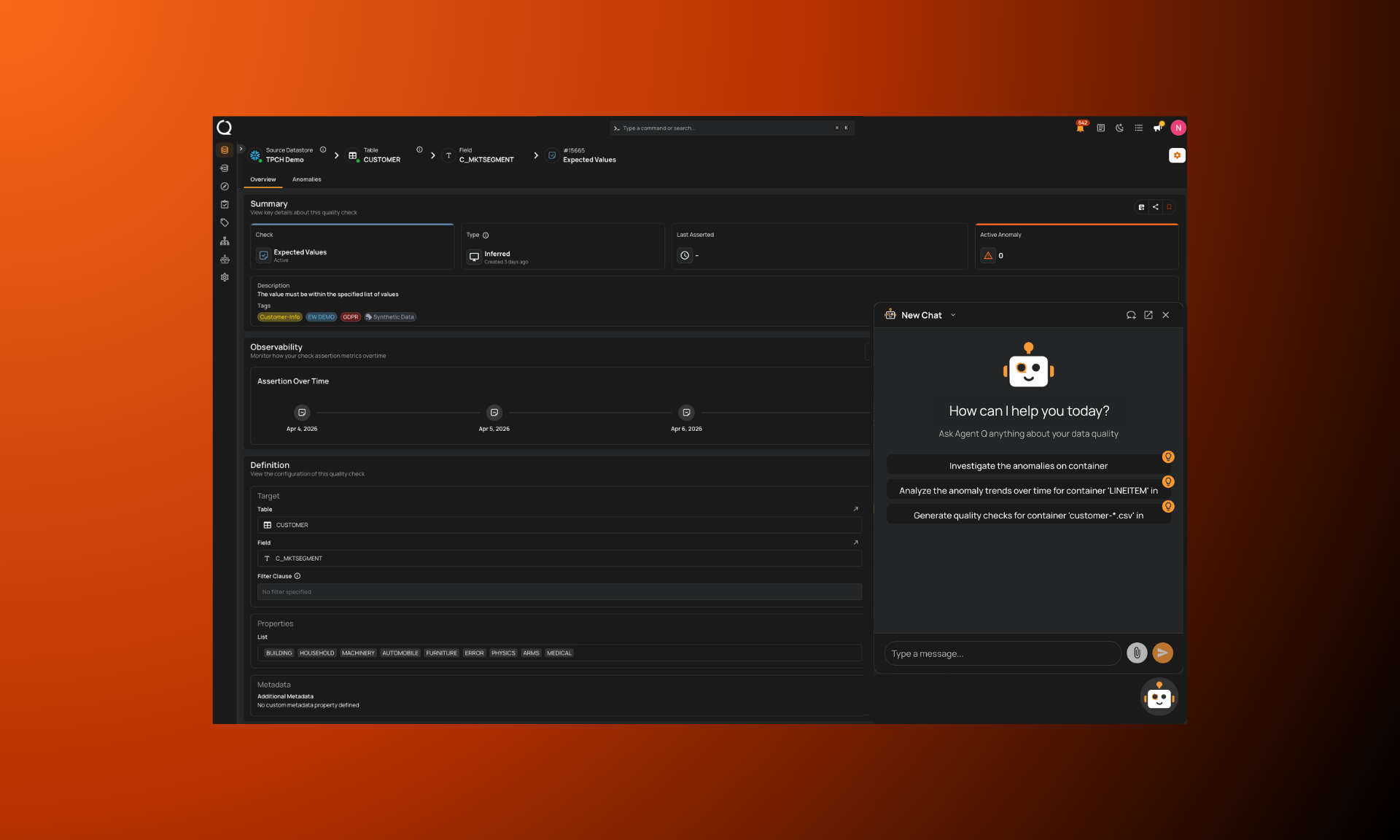
Healthcare payers use Qualytics to enforce data quality upstream: detecting changes the moment new files arrive, resolving fragmented identities before AI acts on incomplete records, validating third-party and EDI data at ingestion, and ensuring the data behind quality scores and compliance reporting is complete. Below are the seven most common ways healthcare organizations operationalize data quality with Qualytics.
Detecting provider file changes before they reach downstream systems
Provider data changes between file deliveries. Providers are added, removed, or modified, and most teams don't discover discrepancies until weeks later when downstream systems break or network adequacy reports come back inaccurate. If you can't consistently identify a provider across your data, you can't accurately pay them, measure them, manage your network, or trust your analytics.
Healthcare payers use Qualytics to automatically profile incoming provider files and run a comparison against the prior baseline. When a stable identifier like NPI is present, the platform matches on it directly. When it isn't, multi-field entity resolution matches providers across name, address, taxonomy, and other attributes, so adds, removes, and field-level changes are detected even when the identifier is missing, reused, or inconsistent between deliveries.
What used to be a manual reconciliation process becomes an automated detection workflow. The team sees that a provider file changed with eight providers impacted and clicks directly to what changed, before any downstream system acts on bad data.
CMS Medicare Advantage directory accuracy requirements and No Surprises Act network adequacy obligations create real regulatory pressure around provider data accuracy. Proactive detection at the file level is the most direct way to stay ahead of it.
Resolving fragmented member identities before AI acts on incomplete records
Member and patient records exist in multiple systems, often with slight name variations, missing identifiers, or incomplete histories. When an AI agent or a live agent using an AI tool queries one system, it may return a single record that's missing critical context. The agent then acts on that incomplete picture, confidently.
Consider this scenario: a customer support AI agent pulls up a member record. The member has called four times, but the complaint history lives in a second record under a slightly different name spelling. The AI reports no prior contact history. The care coordinator proceeds without knowing the full picture.
Healthcare payers use Qualytics to surface records that are likely the same person through entity resolution checks. In a scenario like the one above, two records scored 89% similarity, flagging them as likely duplicates. The Qualytics MCP tool delivers this quality context to the AI agent before it responds, so the agent gets the full picture rather than a confident wrong answer.
Fragmented member identities are a known problem in healthcare, and they become a significantly larger risk when AI systems make care coordination or service decisions on an incomplete record. Multi-field entity resolution matches records across name, identifier, and demographic fields, so the full member picture is assembled before an AI system acts on a partial one.
Validating third-party and EDI data at ingestion
Healthcare organizations ingest large volumes of third-party data: EDI 837 claims feeds, FHIR resources, eligibility files, pharmacy feeds, lab results, and CMS reference files. This data is often consumed across clinical, financial, and operational workflows before anyone has validated it. Schema changes, late deliveries, volume drops, and definition drift from vendors create coverage gaps that aren't discovered until downstream.
A real example: behavioral health providers sometimes submit all their claims in a single batch at month-end. Without volume and freshness monitoring, that spike looks like a data quality anomaly, or the absence of expected data earlier in the month goes undetected entirely.
Healthcare payers use Qualytics to validate third-party data at the point of ingestion. Freshness and volume checks confirm expected delivery cadence and file completeness. Schema drift detection flags structural changes in EDI feeds or vendor file layouts before downstream systems consume them. Cross-field consistency validation ensures that related attributes within claims, eligibility, or pharmacy records align with expected relationships. For EDI-specific feeds, time-series monitoring distinguishes expected batching patterns (such as month-end behavioral health submissions) from genuine data anomalies.
Ensuring claims data integrity for analytics and automation
Claims data is dynamic and sourced from multiple systems. Missing attributes, misclassified procedure codes, or inconsistent claim statuses undermine analytics, reserving, and AI-driven claims workflows. When these issues aren't caught early, they drive rework during financial close, distort loss ratios, and amplify through automated processes.
Healthcare payers use Qualytics to continuously validate claims and transaction data before it feeds analytics or AI-assisted workflows. Domain and validity checks enforce correct classifications, while reconciliation and aggregation checks align claims activity across claims, actuarial, and finance systems.
One global insurer generated over 18,000 inferred rules automatically across 19 million records, saved nearly 3,000 engineering hours, and reduced its data quality timeline from 9-12 months to one week. Underwriters and analysts now write, refine, and validate rules themselves.
Early validation prevents partial or misclassified claims data from being amplified into distorted outcomes by automated systems.
Validating data for HEDIS, STAR ratings, and quality measurement
HEDIS measures and STAR ratings depend on data completeness and accuracy across claims, EHR records, and supplemental sources. Quality scores are performance metrics and financial levers. They directly affect reimbursement rates for providers and health plans. A care gap that goes unclosed because a qualifying claim is missing, miscoded, or misattributed understates a measure and has a direct financial consequence.
The data challenge is that numerator and denominator logic for HEDIS measures pulls from multiple source systems, and those sources are rarely in perfect agreement. Payers that operate across multiple acquired plans or regional systems often have further fragmentation: inconsistent coding standards, different EHR instances, and supplemental data that doesn't reconcile cleanly across populations.
Healthcare payers use Qualytics to validate numerator and denominator completeness across claims, EHR, and supplemental sources. Existence checks confirm that qualifying encounters and procedures are present in the correct source system. Cross-field consistency rules validate alignment between diagnosis codes, procedure codes, and measure-specific attribution logic. Reconciliation checks surface discrepancies between supplemental data submissions and claims-based denominators before they suppress a measure. AI-assisted rule creation enables rapid alignment with evolving measure specifications, reducing the technical lift required when NCQA updates measure definitions year over year.
HEDIS and STAR performance is a data quality problem as much as a clinical one. Organizations that validate the underlying data continuously protect both their quality scores and the financial outcomes tied to them.
Enabling shared ownership between governance and clinical teams
In most healthcare organizations, data quality accountability sits almost entirely with technical teams, even when the people who understand what "good" member or claims data looks like are clinical operations managers, actuaries, compliance officers, or quality analysts responsible for HEDIS reporting. This creates bottlenecks, slows remediation, and produces rules that reflect technical validity rather than clinical or operational reality.
Large health plans compound this further by operating across multiple acquired systems, each with its own data conventions and governance team. Without a shared platform, a rule that exists in one system doesn't exist in another.
Healthcare payers use Qualytics to provide a no-code/low-code environment where governance, clinical operations, quality analytics, and data teams can co-own data quality. Business users, including quality analysts, underwriters, and compliance leads, contribute domain knowledge by defining and refining checks. Data teams maintain scalable frameworks. Both sides work from the same governed foundation, with full auditability.
When only engineers can write rules, the rules don't reflect clinical or operational reality. Shared ownership closes that gap and is the model that makes data quality sustainable at scale.
Producing audit-ready evidence of data controls
Healthcare organizations operate under HIPAA, CMS reporting requirements, and increasingly, state-level health data regulations. Evidence of data quality controls is often fragmented across scripts, logs, and spreadsheets. During audits or regulatory exams, teams reconstruct proof of control execution retroactively, an expensive and error-prone process.
Qualytics retains traceable evidence of data quality control execution: results, failed records, approvals, and remediation history across all data sources. Time-series views demonstrate control effectiveness over time.
Healthcare payers using Qualytics report that audit readiness becomes a byproduct of daily operations rather than a last-minute reconstruction effort.
Proactive data quality and regulatory defensibility are the same capability, not separate workstreams. Organizations that govern data quality continuously don't scramble for evidence when it's requested.
Healthcare payers use Qualytics to enforce trust at scale
Healthcare data quality failures don't announce themselves. They show up in network adequacy reports, compliance findings, denied claims, suppressed HEDIS measures, or an AI system that acts on stale, fragmented, or unvalidated data. By then, the cost of remediation is orders of magnitude higher than the cost of prevention.
Organizations that enforce data quality upstream, validating at ingestion, detecting changes immediately, resolving identities before AI acts on them, and ensuring the data behind quality scores is complete, build a foundation that scales with automation rather than eroding under it.
Book a demo to see how healthcare organizations operationalize data quality with Qualytics.
Chapters
Related Articles

Data Quality vs Data Control: Why AI Demands Controls
AI removes the human safety net that contained bad data. The data control layer validates data at the moment it's acted on.

How Insurers Enforce Data Quality Before It Impacts Premiums, Claims, and Compliance
Insurance companies use Qualytics to operationalize proactive data quality to protect premiums, underwriting, claims, and regulatory reporting—preventing amplifying hidden data issues into financial and compliance risk.
Qualytics Introduces the Data Control Layer for Trusted Context
AI systems depend on context, but context without control creates risk. Qualytics introduces the data control layer that enables trusted data at the moment it is used.
Related News
Data Quality vs Data Control: Why AI Demands Controls
AI removes the human safety net that contained bad data. The data control layer validates data at the moment it's acted on.
How Insurers Enforce Data Quality Before It Impacts Premiums, Claims, and Compliance
Insurance companies use Qualytics to operationalize proactive data quality to protect premiums, underwriting, claims, and regulatory reporting—preventing amplifying hidden data issues into financial and compliance risk.
Qualytics Introduces the Data Control Layer for Trusted Context
AI systems depend on context, but context without control creates risk. Qualytics introduces the data control layer that enables trusted data at the moment it is used.